
The LDL Paradox
Understanding cardiovascular risk when symptoms are absent

Gather any group of people of around a certain advanced age, and inevitably the topic of conversation turns to health. The last dinner party I attended was no exception. Somehow we started talking about heart disease and the causal role of low-density lipoproteins (LDLs). Peter Libby, one of the leading authorities on cardiovascular disease, wrote in Nature in 2021:
LDL, a particle encircled by its signature apolipoprotein B component, causes atherosclerosis. If the entire population maintained LDL concentrations akin to those of a neonate (or to those of adults of most other animal species), atherosclerosis might well be an orphan disease.
An orphan disease is one in which there are so few cases on the planet that people do not know what it is. Instead, atherosclerotic cardiovascular disease (ASCVD) is the number one killer of both men and women in the developed world with nearly twenty million global fatalities per year. Women in the U.S. are 10 times more likely to die of heart disease than breast cancer.
A friend of mine then told me she had high levels of LDL but apparently no evidence of heart disease within the last five years. “How do you explain that?” she asked. I didn’t have a good answer at the dinner party, so I wrote this post to help clarify my thinking and provide some answers to her question. First I’ll summarize the key cardiovascular research data linking LDL to heart disease. Then I’ll explore some of the reasons my friend might not show signs of heart disease despite her high levels of LDL.
Root Cause of Heart Disease
Atherosclerosis is a slow, progressive disease where plaque builds up inside artery walls, causing them to harden and narrow. The plaque buildup restricts oxygen-rich blood flow to tissues, often leading to heart disease, stroke, or peripheral artery disease.
The key events in the initiation of ASCVD are the retention and accumulation of cholesterol-rich apolipoprotein B (apoB) containing lipoproteins within the inner lining of the arteries at sites susceptible to plaque formation. All lipoprotein particles are wrapped by large molecules called apolipoproteins. High-density lipoproteins (HDL) particles are wrapped by one or more apolipoprotein A (apoA) particles. All of the non-HDL particles are wrapped by only one apoB particle. Both apoA and apoB-containing lipoproteins are very small and can efficiently penetrate the arterial lining. Importantly, apoB-containing lipoproteins are far more likely to get stuck inside the arterial lining than apoA-containing lipoproteins. Under the right conditions, some of these apoB particles are retained in the arterial wall, leading to the initiation and progressive development of atherosclerotic plaque.
ApoB-containing lipoproteins include LDL, VLDL, IDL, their remnants, and Lp(a). In most people, LDL particles represent 90% of circulating apoB-containing lipoproteins in fasting blood. In practice, the number of LDL particles is not measured directly but instead estimated from its cholesterol concentration (LDL-C). As a result, calculated plasma LDL-C has become the most common measure for assessing cardiovascular risk and for evaluating therapeutic benefit in randomized clinical trials.
A 2017 meta-analysis of over 200 genetic studies, prospective epidemiologic studies, Mendelian randomization studies, and randomized clinical trials including more than 2 million participants with over 20 million person-years of follow-up and over 150,000 cardiovascular events provided remarkably consistent and unequivocal evidence that LDL causes ASCVD. Figure 1 shows the dose-dependent log-linear association between the magnitude of change in LDL cholesterol (LDL-C) and the reduction in risk of ASCVD relative to the control group.
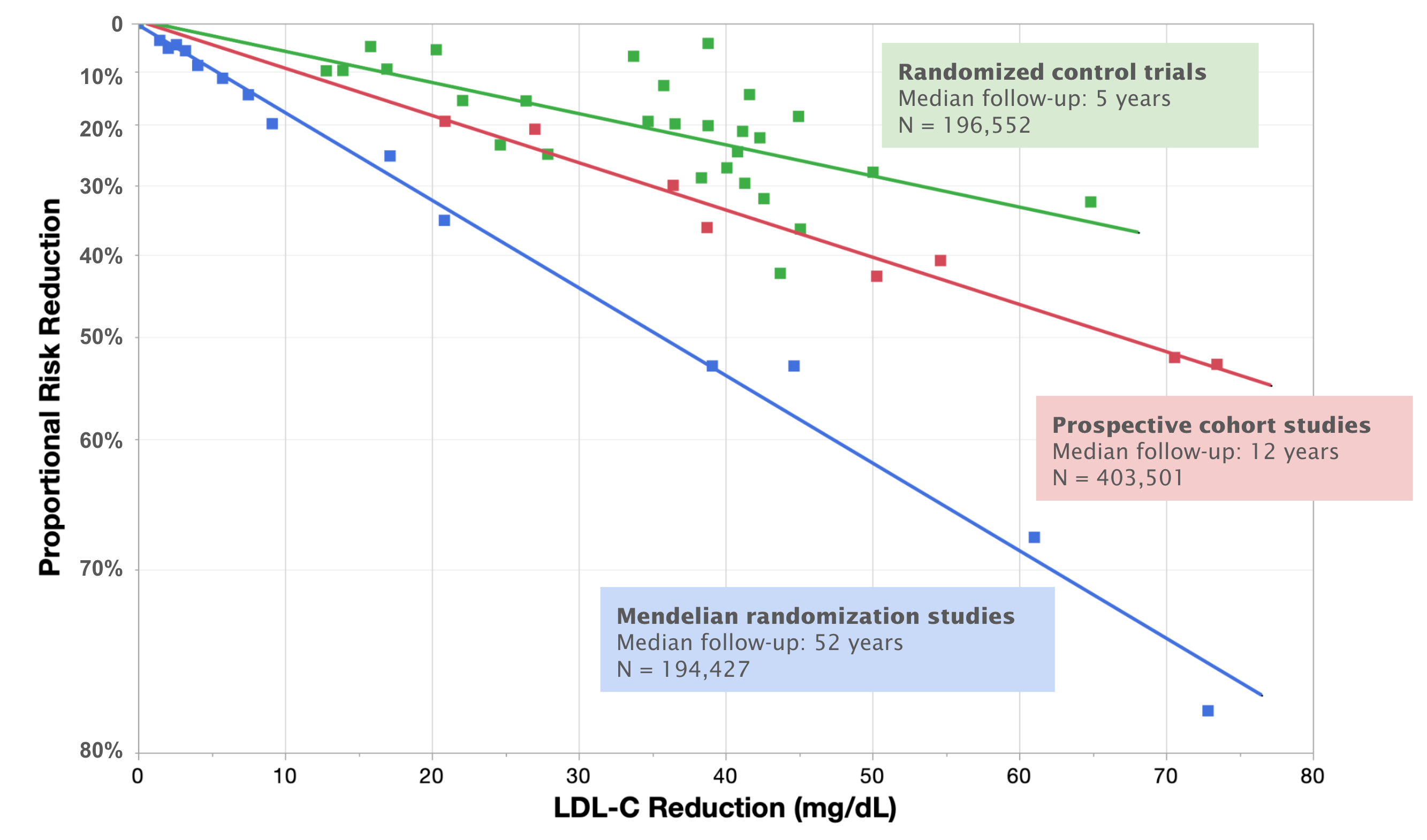
Fig. 1. Log-linear association per unit change in low-density lipoprotein cholesterol (LDL-C) and the proportional risk reduction of cardiovascular disease.
Two things are evident from this chart. First, the greater the reduction of LDL-C, the lower the risk of heart disease relative to the control group. Second, the longer period of time over which the reduced LDL-C levels are maintained, the lower the risk of heart disease. Five years of treatment with a lipid-lowering agent that lowers LDL-C by about 40 mg/dL should reduce the relative risk of ASDVD by 20-25%. Fifty years of exposure to 40 mg/dL lower LDL-C would be expected to reduce ASCVD events by 50-55%. Both results are consistent with a mechanism where the number of apoB-containing particles and the time they are circulating influence the risk of ASDVD.
In these studies, LDL-C and apoB concentrations had very similar effects on the risk of cardiovascular events, thus confirming that LDL-C is a satisfactory surrogate for LDL particle number under most circumstances. However, in certain conditions (e.g. metabolic syndrome, diabetes, and hypertriglyceridaemia), plasma LDL-C may not accurately reflect LDL particle concentration or its effect on cardiovascular risk. Recent studies have demonstrated that apoB concentration is a more accurate indicator of ASCVD risk than LDL-C. Thus anyone concerned about ASCVD risk should have their apoB concentration measured to account for potential discordance with LDL data.
Explain That…
Given the evidence that LDL causes atherosclerosis, how can my friend have high levels of LDL and an apparent lack of disease? I think the most relevant explanation is time. Atherosclerosis is a cumulative, dose-dependent disease. Having no apparent disease today does not mean there is no developing risk. Think of ASCVD risk like smoking. You don’t get lung cancer after one cigarette; you get it after decades of exposure. Exposure to high levels of apoB-containing particles is a “dose” of risk that accumulates every single day they stay elevated.
Consider the data shown in Figure 2. This study looked at a population of 1,779 adults without conventional cardiovascular risk factors (absence of dyslipidemia, hypertension, diabetes, and smoking). The average participant was 45 years old with nearly the same number of males and females in the study. Ultrasound was used to measure plaque in the carotid, iliofemoral, and abdominal arteries and coronary artery calcification. As LDL-C levels increased, there was a linear increase in the presence of atherosclerosis even in apparently healthy individuals without conventional risk factors. The population with detectable plaque ranged from 11% in the 60-70 mg/dL subgroup to 64% in the 150-160 mg/dL subgroup.
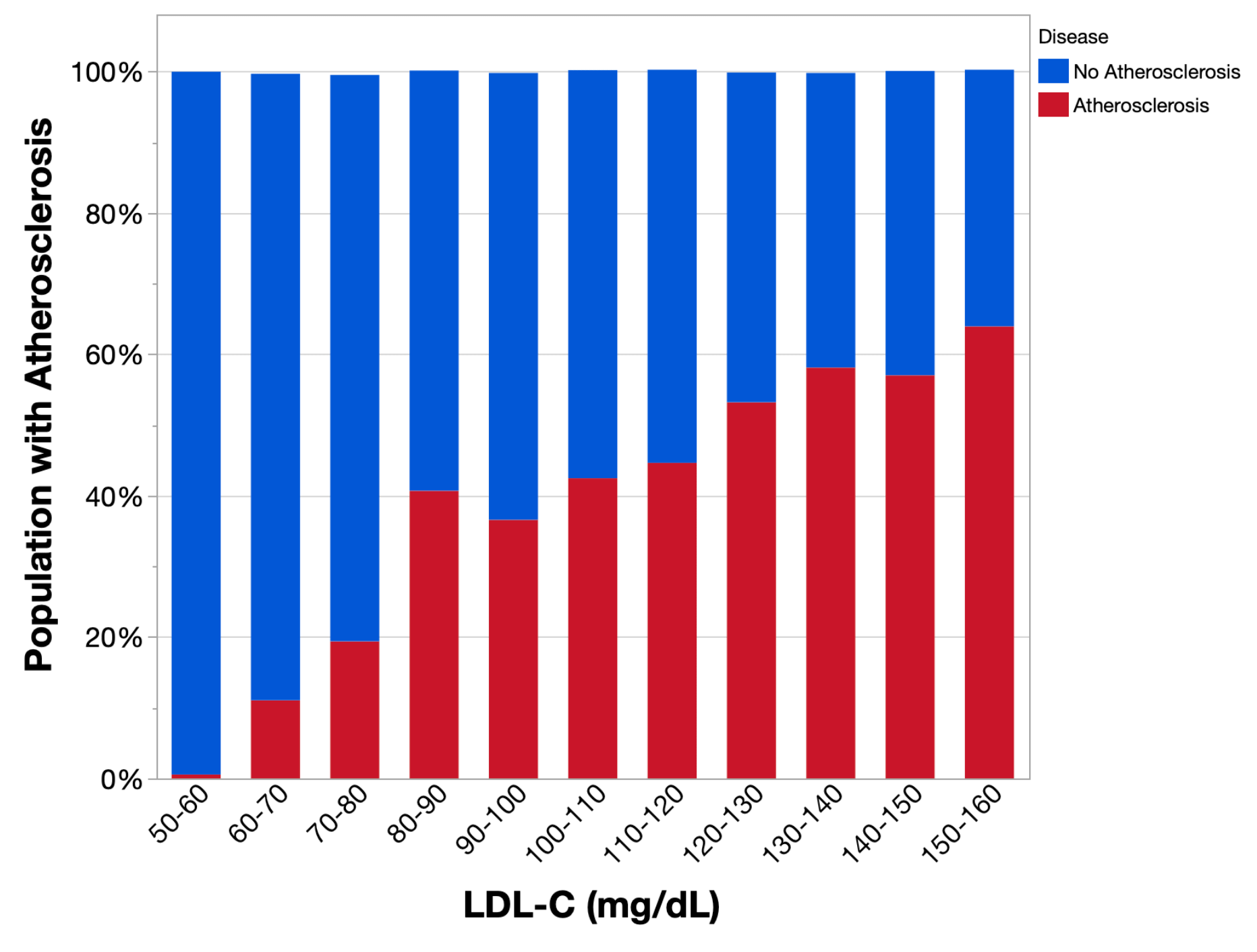
Fig. 2. Relation between LDL-cholesterol levels and atherosclerosis in healthy individuals without conventional cardiovascular risk factors.
My friend told me that her non-HDL cholesterol was 165 mg/dL. We can estimate her LDL-C by assuming that 90% of her non-HDL-C is LDL-C, which is typical for most people. Using this assumption, my friend’s LDL-C concentration is about 150 mg/dL. At this level, about 60% of 45 year old healthy individuals have detectable atherosclerosis in their arteries, but 40% do not have detectable atherosclerosis.
This just shows that LDL particles are necessary for disease progression but do not guarantee the presence of disease. Some people have resilient artery walls or favorable blood flow dynamics that resist plaque formation longer than others, so called “parietal factors.” Inflammation is another factor that influences plaque formation. Several recent trials showed that reducing inflammation reduces cardiovascular events even without changing lipid levels. Think of apoB-containing particles as the “seed” and inflammation as the “soil.” If a person’s systemic inflammation is low, those “seeds” might not have the right environment to grow into plaques yet, but the seeds are still being planted. Other factors like disturbed sleep, physical inactivity, the microbiome, air pollution and environmental stress may also play a role in how fast plaque forms.
Nonetheless, the probability that an apoB-containing particle will be retained within the arterial lining leading to the development and growth of plaque increases with both the total amount of circulating particles and on the length of time those particles are circulating. One study showed that the risk of a future ASCVD event at a given age increases with cumulative prior exposure to LDL-C. This study included 4,958 asymptomatic adults aged 18 to 30 years. During a median 16-year follow-up after age 40 years, 275 participants had an ASCVD event. ASCVD events included nonfatal coronary heart disease, stroke, transient ischemic attack, heart failure hospitalization, cardiac revascularization, peripheral arterial disease intervention, or cardiovascular death. Figure 3 compares the ASCVD event results for the lowest and highest quartile of LDL-C exposure prior to age 40. The lowest quartile represents a person exposed to LDL-C concentration below about 96 mg/dL from age 18 to 40. The highest quartile represents a person exposed to LDL-C concentration above about 130 mg/dL from age 18 to 40. At age 55, 8.6% of the highest quartile participants suffered a cardiac event, while only 2.6% of the lowest quartile participants had suffered an event. Incident ASCVD event risk depends on cumulative prior exposure to LDL-C, illustrating the importance of optimal LDL-C control starting early in life.
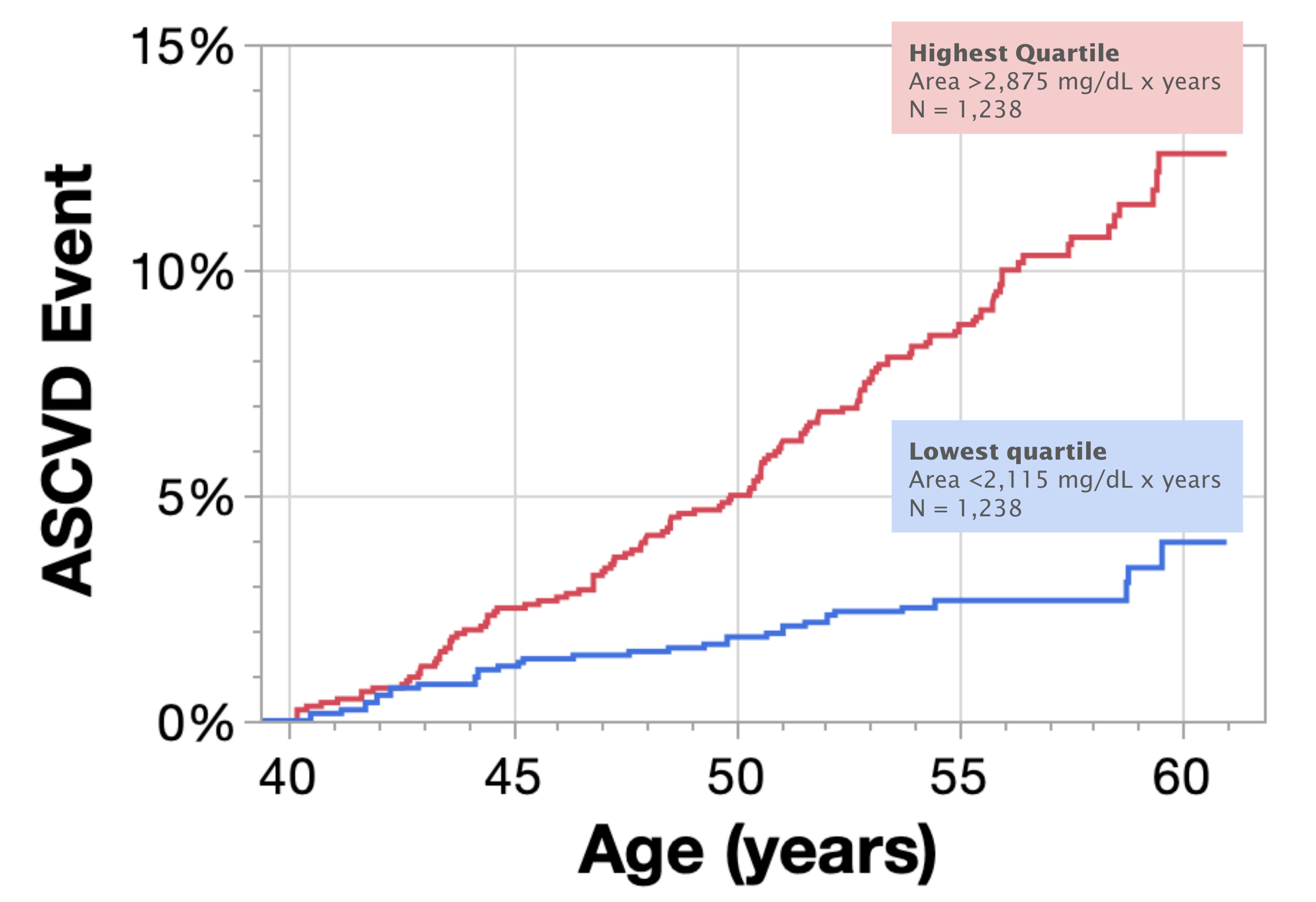
Fig. 3. ASCVD events in participants exposed LDL-C concentrations equivalent to <96 mg/dL (lowest) and >130 mg/dL (highest) for 22 years before the age of 40.
The Bottom Line
High levels of apoB-containing particles like LDL are necessary but not sufficient to cause heart disease. The risk is cumulative and dose dependent, meaning that higher exposure over longer time horizons leads to the greatest risk. The data is clear: the more apoB particles you have circulating, the higher the risk, regardless of how you feel today.